|
|
Health Equity Framework |
|
|
IN THIS SECTION
The Health Equity Framework Social Determinants of Health Social Determinants of Health Equity |
Although the terms “disparity,” “inequality,” or “inequity” may be used somewhat interchangeably (click here for definitions), a shift to a health equity framework is particularly meaningful and an important foundation of this guide. Healthy People 2020 defines health equity as “attainment of the highest level of health for all people.” This shift is more than semantics and is distinguished from a disparities-driven approach in several important ways.
|
An equity framework draws attention to the concepts of fairness and justice in the distribution of resources. Furthermore, it highlights the idea that social inequities in health are avoidable through collective action and that inaction is unacceptable. In addition, a health equity framework provides a positive vision to work towards—it is inclusive, affirming, and empowering.
Importantly, achieving health equity does not necessarily mean seeing equal outcomes across the population. For Example, the Delaware Division of Public Health envisions “health equity for all Delawareans, where everyone will achieve their full health potential.” This is important as the full health potential for one individual may be different than that of another due to genetic or biological factors, for instance.
A health equity framework draws attention to the need for equity in access to and quality of the resources needed for health and moves away from a disease-specific or individual risk factor orientation. Some experts have referred to this as needing to “create a level playing field” (Knight, 2014). Achieving health equity requires a greater focus on improving underlying social and economic conditions, such as income and education. These conditions are structural and systemic in nature, much like the strong bridges and fences of the stream parable. In essence, a health equity lens moves us farther upstream to address the social determinants of health and health equity.
Social Determinants of Health
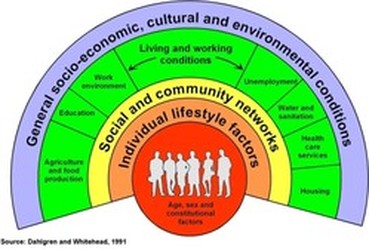
Fig. 1: Social Determinants of Health & Levels of Influence (Dahlgren & Whitehead, 1991) |
The social determinants of health (SDOH) are often defined as the circumstances in which people are born, grow up, live, work, and age. The World Health Organization (WHO) explains that these circumstances are in turn shaped by a wider set of forces: economics, social policies (such as education, social security and welfare), and politics (including power and decision-making). This understanding of the SDOH is important in relation to health equity, as it recognizes that economic, social and political conditions are not naturally occurring. Instead, these conditions are the result of public policy and other community or collective actions. Therefore, the SDOH are rooted in long-term structures and traditions that may be resistant to change.
Health equity is about fairness and justice, and is indistinguishable from equity generally." (Knight, 2014) |
|
Efforts to define, understand, and address the SDOH have been growing since the 1990s. Various research organizations and public health institutions have sought to identify the various social influences on health and explain their relations with population health and the health of specific population groups. Conceptual frameworks were developed to help explain levels of influence and identify opportunities for intervention. One such model, developed by Dahlgren and Whitehead at the forefront of the field (see Figure 1 above), is frequently used to describe the various determinants of health. The model highlights levels of influence, with the most distal factor, the prevailing socioeconomic and cultural conditions, as the very structure of society in which each of the other levels function. The model puts living and working conditions, such as housing and education, within the context of these societal structures, suggesting that they are not naturally occurring conditions. Rather, living and working conditions come about as a result of overall societal structure, culture, and both historic and current public policies. Another way of thinking about this is that living and working conditions are not inevitable; they are amenable to change. The model also highlights the fact that individual behavior and lifestyle choices are made within the context of one’s social and community networks as well as the broader environment.
Attention to the SDOH has grown substantially in the United States in recent years. A major goal within Healthy People 2020 is to “create social and physical environments that promote good health for all.” Healthy People 2020 distinguishes between social and physical determinants in the environment but recognizes their interrelated nature in contributing to the places where people are born, live, learn, work, play, worship, and age. |
Many lists of determinants and variations on the rainbow model originally presented by Dahlgren and Whitehead have been created in recent years and used for different purposes (See Figure 2 below). Experts continue to learn more about the ways in which social conditions impact health; models are improving to reflect this enhanced understanding. Notwithstanding such scientific advances and differences in purpose among varied approaches, it is important to recognize that all of the lists, frameworks, and models describing the SDOH in recent years share key elements that are critical for health promotion:
|

Fig. 2: Conceptual Framework for the Determinants of Health Equity
Source: World Health Organization, 2010 |
Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and healthcare disparities.” (Healthy People 2020) |
Figure 2, reproduced from the WHO report mentioned above, illustrates this understanding regarding the structural determinants of the social determinants of health. This figure is useful for highlighting the need to move even farther upstream. Living and working conditions, described as SDOH, are viewed as more proximate to health and equity, whereas macroeconomic policies and other social policies—housing, education, and social security—are further upstream. Figure 2 illustrates how these policies—along with culture, societal values, and governance—are related to socioeconomic position and result in inequities between groups of people categorized by gender, race, and class. Meaningful, long-term changes that promote health equity are needed farther upstream at that structural level—identified in Figure 2 as being within the socioeconomic and political context—in a health equity framework.
Our approach is based on a comprehensive model developed by the Bay Area Regional Health Inequity Initiative. This model is represented in the figure 3 below. For more detail on how this guide is structured around this framework, please refer to our Health Equity Lens Page

Figure 3 Public Health Framework for Reducing Health Inequities
Social Determinants of Health Equity
In 2008, the WHO Commission on the Social Determinants of Health published a ground-breaking report on health inequities, which summarized decades of research from around the world. The report explained that differences in SDOH are mostly responsible for health inequities. Available data on the SDOH indicate that social advantages and disadvantages are relative. For example, individuals who experience extreme poverty are more likely to experience poor health than those who have even slightly more resources, while those at the highest socioeconomic level are generally the healthiest. The same pattern holds for education level and other indicators of social status. Furthermore, the effects of these factors can be cumulative. For example, individuals who are poor, Black, and have low levels of education are more likely to be in poor health than someone who has just one or two of those characteristics.
Importantly, the WHO report (and numerous related publications) point out that differences in the SDOH that underlie health inequities are themselves socially determined. In other words, the working and living conditions that determine health and health inequities are not naturally occurring. Instead, they are determined by policy decisions and other social structures and actions (e.g. media, business, etc.) that affect communities and societies at large.
Importantly, the WHO report (and numerous related publications) point out that differences in the SDOH that underlie health inequities are themselves socially determined. In other words, the working and living conditions that determine health and health inequities are not naturally occurring. Instead, they are determined by policy decisions and other social structures and actions (e.g. media, business, etc.) that affect communities and societies at large.
