
|
|
Upstream Strategies for Community Health |
|
|
|
Upstream strategies target a continuum of health equity, which includes the physical, social, economic and work, and service environment through community capacity building, community organizing, and civic engagement. This is pictorially represented in the Public Health Framework for Reducing Health Inequities (Figure 1) Related strategies include building strategic partnerships and engaging in advocacy to change the underlying structures that determine living conditions.
"Like a truly healthy human body, a truly healthy community is one in which all systems function as they should, and work together to make the community function well. In an individual, health is, to a large extent, a result of all the body’s billions of cells getting what they need. For a community, health is, to a large extent, the result of all citizens getting what they need, not only to survive, but to flourish.” |
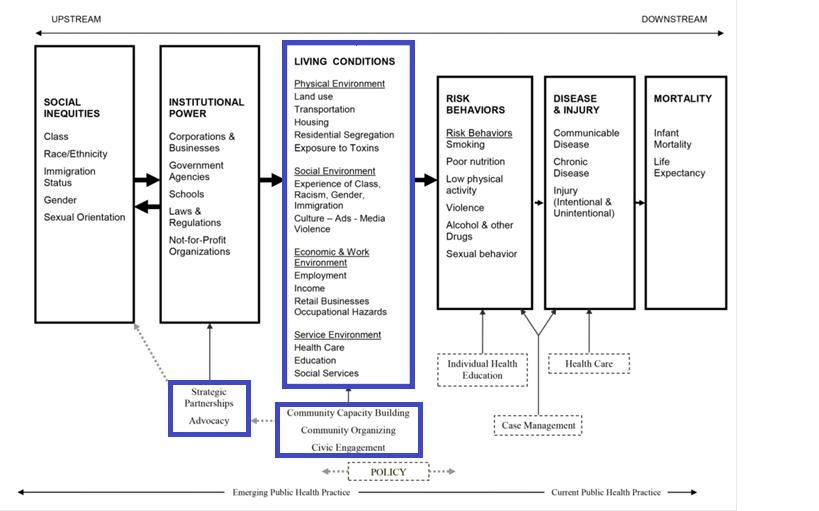
Fig. 1: Public Health Framework for Reducing Health Inequities
|
Improvement of living conditions can help create healthy communities and, ultimately, improve health equity. A healthy community is one that continuously improves its physical and social environments, thereby helping people to support one another to develop to their fullest potential. In other words, a healthy community is one in which all of its residents have the resources needed to thrive: clean air and water, parks and green space, healthy food, affordable housing, jobs and income, transit, and positive social interactions. For everyone to thrive, a healthy community must also include social justice, equity, and sustainable resources. A healthy community must be free of all forms of discrimination and allow everyone an opportunity to participate in its governance.
1. Defining "Communities"
Communities can be defined in many different ways. Traditionally, communities are conceptualized as geographic areas. In terms of healthy equity, communities are often defined broadly and can also refer to groups of people that share certain characteristics, values, or a common social identity. Furthermore, a community is often best defined by the members of that community. While we appreciate the importance of various definitions of community, for the purposes of this guide, we draw attention to the geographic definition of community and the idea that communities are physical places. Growing evidence suggests that there are healthy places to live and less healthy places to live. Furthermore, the differences between healthy and less healthy places cannot be explained by the characteristics of the people living in those places, such as income or race. According to the Centers for Disease Control and Prevention (CDC), healthy places are those designed and built to improve the quality of life for all people who live, work, worship, learn, and play within their borders–where every person is free to make choices amid a variety of healthy, available, accessible, and affordable options. The conceptualization of healthy communities is what led to the eventual development of place-based initiatives as a means to improve community health.
|
Regardless of whether a community is healthy or less healthy, opportunities for improvement exist across the continuum. Given what we know about the social gradient in health and the social determinants of health (SDOH), everyone can be healthier. Therefore, every community holds the potential to be a healthier place to live. Understandably, some health professionals become overwhelmed by the complex web of challenges and apparent disadvantages in less healthy communities. But those communities simply have more areas for improvement.
|
A seemingly modest change can build upon itself or be leveraged to promote greater changes and impact. An investment in one area can stimulate investments in other areas. A new playground that brings families together can inspire an adjacent community garden. Removing graffiti and improving the lighting along a sidewalk invites people outside, simultaneously discouraging vandals and other criminal activity. And a new corner store can encourage additional commercial activity and investment.
|
2. Place Based Initiatives
Health-oriented strategies that are focused on living conditions in specific communities are often described as “place-based initiatives” (PBIs) because the target of the interventions is the place itself (or characteristics of the place), rather than the people living in that place. For instance, place-based strategies to address obesity may include working with fast-food establishments to offer healthy food options as opposed to more traditional people- or population-based approaches, such as health education to change eating habits. Comprehensive approaches recognize that both place-based and people-based strategies are important, and this is reflected in Figure 1. However, PBIs are generally considered to be more effective at addressing underlying root (upstream) causes of unhealthy behaviors. Although, PBIs are not exclusive to health (click here to read more), we draw special attention to them because they address the health inequities we currently see in the distribution of resources and hazards across communities.
The Department of Education’s Promise Neighborhoods initiative exemplifies the Obama Administration’s attention to PBIs, by focusing resources on a comprehensive range of factors in the community that lead to better educational outcomes. Similarly, the Department of Housing and Urban Development’s Choice Neighborhoods initiative is aimed at transforming poor neighborhoods into places with sustainable, mixed-income housing. Importantly, both of these initiatives support locally-driven, collaborative strategies for improving community conditions to address complex social problems.
The Department of Education’s Promise Neighborhoods initiative exemplifies the Obama Administration’s attention to PBIs, by focusing resources on a comprehensive range of factors in the community that lead to better educational outcomes. Similarly, the Department of Housing and Urban Development’s Choice Neighborhoods initiative is aimed at transforming poor neighborhoods into places with sustainable, mixed-income housing. Importantly, both of these initiatives support locally-driven, collaborative strategies for improving community conditions to address complex social problems.
Characteristics of Place-Based Initiatives for Health and Health Equity
- a concentration of resources and interventions in a defined geographic area
- integrated and holistic approaches to addressing the determinants of health
- an investment in early intervention and prevention
- multi-sector participation and collaboration
- community engagement, participation, ownership, and leadership
- a good understanding of the community (needs, resources, priorities, etc.)
- a focus on long-term and sustainable changes
- advocacy and policy change.
Dimensions of Place-Based Initiatives
As highlighted in Figure 1 (shown above), four main dimensions of the environment fall under the heading of “living conditions,” and they account for the most critical levers of meaningful change at the local level. We describe the relations between each dimension and health equity, along with strategies for improving conditions in each dimension.
The four dimensions of healthy communities—the physical, social, economic and work, and service environments, discussed in depth below, are interrelated and interdependent. Many of the risk and protective factors described could fit within multiple dimensions (e.g. parks could be described within the physical environment as well as the service environment). Similarly, the strategies highlighted for each dimension are likely to have positive impacts across other dimensions. It is unnecessary to specify or prioritize a dimension when promoting place- based initiatives. Rather, the distinctions among the four dimensions are intended to organize the discussion and can be useful in identifying areas for intervention.
Physical Environment
The physical environment includes both the natural environment (i.e. parks and green space) and the built environment (i.e. roads and sidewalks). The physical environment can influence health directly. For instance, the quality of the air we breathe can be directly linked to asthma rates, such that people living in poorer air quality areas (such as near highways) experience higher rates of asthma. The physical environment also impacts health indirectly by influencing health-related behaviors. For instance, the existence of sidewalks and bike lanes can promote physical activity, while poor lighting or graffiti can discourage people from being outside.
Healthy places have an abundance of health protective, or health promoting, factors such as safe parks and green space, walkable neighborhoods, quality mixed-income and racially diverse housing, healthy food outlets, public transportation, and access to other kinds of community resources that encourage residents to gather together socially. In contrast, unhealthy places tend to be characterized by risk, or health damaging, factors such as substandard housing and residential segregation, abandoned buildings and lots, run-down or non-existent sidewalks and parks, toxic environmental exposures (i.e. lead or air pollution), physical barriers for people with disabilities, and a high concentration of tobacco, alcohol, and fast food retailers.
The quality of the physical environment—natural and built—varies from place to place, which contributes to health inequities along geographic lines. For this reason, Healthy People 2020 emphasizes improving neighborhood living conditions to promote health equity.
Healthy places have an abundance of health protective, or health promoting, factors such as safe parks and green space, walkable neighborhoods, quality mixed-income and racially diverse housing, healthy food outlets, public transportation, and access to other kinds of community resources that encourage residents to gather together socially. In contrast, unhealthy places tend to be characterized by risk, or health damaging, factors such as substandard housing and residential segregation, abandoned buildings and lots, run-down or non-existent sidewalks and parks, toxic environmental exposures (i.e. lead or air pollution), physical barriers for people with disabilities, and a high concentration of tobacco, alcohol, and fast food retailers.
The quality of the physical environment—natural and built—varies from place to place, which contributes to health inequities along geographic lines. For this reason, Healthy People 2020 emphasizes improving neighborhood living conditions to promote health equity.
Sample Strategy
Asthma disproportionately affects low-income children due to the poor air quality in their homes, schools, and neighborhoods. Indoor and outdoor triggers and pollutants cause trips to the emergency room and school absences. In urban areas, diesel particles from ports and heavy traffic have been linked to worsening asthma. Across the country, communities are addressing this issue by improving public transportation and holding industries and governments more accountable for environmental impacts, particularly concerning air quality. Indoor air quality is being improved by enhancing ventilation in older school buildings and enforcing housing codes in low-income housing residences.
In June 2014, the Delaware Division of Public Health (DPH) launched the Healthy Homes initiative in partnership with Nemours Health and Prevention Services and four housing authorities. The initiative aims to reduce asthma triggers while promoting healthier and safer home environments in targeted communities. The program educates families and provides tools to create and maintain home environments free of common contaminants. Pilot programs are also underway in each of Delaware’s three counties to provide training and technical assistance to local housing authorities. Representatives from the Wilmington Housing Authority, the Delaware State Housing Authority, the Dover Housing Authority, and a privately owned and managed housing agency in Laurel receive several hours of training and technical assistance. The pilot programs support the development of integrated pest management plans at the building level, which expands upon the training and resources offered to individual families. In this way, the Healthy Homes initiative contributes to a healthier physical environment.
For more information and examples of efforts to address childhood asthma, as well as other strategies for improving the physical environment, click here . For more about Delaware’s Healthy Homes initiative, click here.
In June 2014, the Delaware Division of Public Health (DPH) launched the Healthy Homes initiative in partnership with Nemours Health and Prevention Services and four housing authorities. The initiative aims to reduce asthma triggers while promoting healthier and safer home environments in targeted communities. The program educates families and provides tools to create and maintain home environments free of common contaminants. Pilot programs are also underway in each of Delaware’s three counties to provide training and technical assistance to local housing authorities. Representatives from the Wilmington Housing Authority, the Delaware State Housing Authority, the Dover Housing Authority, and a privately owned and managed housing agency in Laurel receive several hours of training and technical assistance. The pilot programs support the development of integrated pest management plans at the building level, which expands upon the training and resources offered to individual families. In this way, the Healthy Homes initiative contributes to a healthier physical environment.
For more information and examples of efforts to address childhood asthma, as well as other strategies for improving the physical environment, click here . For more about Delaware’s Healthy Homes initiative, click here.
Social Environment
The social environment refers to the relationships between community members and the factors that affect those relationships. Places where residents work together, welcome diversity, and have a strong sense of community are places with social capital. Social capital is the strength of relationships among community residents, and is a protective factor. Strong social ties, community cohesion, and civic participation promote health and equity. A well-known study about the 1995 heat wave in Chicago that resulted in hundreds of deaths, particularly among the elderly, revealed that residents of neighborhoods with low levels of social capital were much more likely to die than residents of neighborhoods with high levels of social capital (Klinenber, 2002). Elderly survivors had neighbors and friends to check on them and provide assistance, whereas the deceased were often isolated and lived in areas that lacked social cohesion.
Social capital may also be viewed in terms of the collective identity of a neighborhood and the sense of solidarity that such a collective identity can promote. This is important from the standpoint of health equity because it supports and enhances community empowerment and collective action. The presence of social capital in this regard may be directly associated with community residents’ control over the decisions that affect their living conditions because it strengthens their positions with businesses or institutions that may put the community at risk. For example, when a landlord threatens to displace tenants by increasing rent beyond what is affordable for residents, members of tenant associations can organize to resist such a change that would harm their community. Similarly, strong social capital is appealing to businesses and others considering investments in the community. Like neighborhood beautification projects, social capital is attractive.
Conversely, social segregation, lack of community cohesion, and weak ties put communities at risk for disinvestment and threaten community well-being. Communities with limited social capital are less likely to organize and advocate for themselves. They may also experience more crime and may be viewed negatively by those outside of the community. All of these contribute to disinvestment, lack of resources, and discrimination. According to Bell and Rubin (2007):
“The impacts of a community’s social environment on health run the gamut from psychological to political, with consequences for the physical and economic environments. A community with strong social networks is better able to advocate for itself, its residents better able to control their individual and collective futures” (p. 31).
Social capital may also be viewed in terms of the collective identity of a neighborhood and the sense of solidarity that such a collective identity can promote. This is important from the standpoint of health equity because it supports and enhances community empowerment and collective action. The presence of social capital in this regard may be directly associated with community residents’ control over the decisions that affect their living conditions because it strengthens their positions with businesses or institutions that may put the community at risk. For example, when a landlord threatens to displace tenants by increasing rent beyond what is affordable for residents, members of tenant associations can organize to resist such a change that would harm their community. Similarly, strong social capital is appealing to businesses and others considering investments in the community. Like neighborhood beautification projects, social capital is attractive.
Conversely, social segregation, lack of community cohesion, and weak ties put communities at risk for disinvestment and threaten community well-being. Communities with limited social capital are less likely to organize and advocate for themselves. They may also experience more crime and may be viewed negatively by those outside of the community. All of these contribute to disinvestment, lack of resources, and discrimination. According to Bell and Rubin (2007):
“The impacts of a community’s social environment on health run the gamut from psychological to political, with consequences for the physical and economic environments. A community with strong social networks is better able to advocate for itself, its residents better able to control their individual and collective futures” (p. 31).
Sample Strategy
Urban agriculture and urban farms not only improve economic and health outcomes among low-income families but also foster a sense of community. Community gardens have recently gained popularity through First Lady Michelle Obama’s “Let’s Move!” campaign. Community gardens are believed to reduce obesity and other chronic diseases by improving diets among low-income residents. Community gardens provide a unique opportunity to engage vulnerable individuals—including youth, people who are homeless, and those who are incarcerated—in valuable job training. Residents involved with urban farms can generate supplemental income by selling produce through farm stands, Community-Supported Agriculture (CSA) programs, and at farmers’ markets. Community gardens transform vacant urban spaces into safe green spaces and link different sectors of the community to achieve common goals.
In Delaware, beginning in 2014, Kent Gardens brings together businesses, non-profit organizations, and individuals to build community gardens in Kent County. Partners include: the City of Dover, Delaware Electric Cooperative, Delaware State University, Dover High School, Dover Housing Authority, 4-H, Kent Kids Coalition, Greater Kent Committee, Lowes, Nemours Health and Prevention Services, and many others. The initiative brings the community together to provide healthy food for local residents. In addition, the gardens serve as an avenue to teach children where their food comes from and the importance of agriculture. Community gardens are located in Simon Circle, Kirkwood, Manchester Square, Owens Manor, and Dover High School. These efforts represent community assets that improve the social environment and promote health equity. More information about Kent Gardens can be found here. For examples of other kinds of community garden projects, as well as other strategies for improving the social environment, click here.
In Delaware, beginning in 2014, Kent Gardens brings together businesses, non-profit organizations, and individuals to build community gardens in Kent County. Partners include: the City of Dover, Delaware Electric Cooperative, Delaware State University, Dover High School, Dover Housing Authority, 4-H, Kent Kids Coalition, Greater Kent Committee, Lowes, Nemours Health and Prevention Services, and many others. The initiative brings the community together to provide healthy food for local residents. In addition, the gardens serve as an avenue to teach children where their food comes from and the importance of agriculture. Community gardens are located in Simon Circle, Kirkwood, Manchester Square, Owens Manor, and Dover High School. These efforts represent community assets that improve the social environment and promote health equity. More information about Kent Gardens can be found here. For examples of other kinds of community garden projects, as well as other strategies for improving the social environment, click here.
Economic and Work Environment
The economic and work environment is closely linked with physical and social environments, considering that businesses are necessary to provide jobs and support parks, healthy foods, and other retail establishments. Having a strong business sector is a protective factor in that it promotes financial security among residents through living wage jobs, it encourages homeownership, and it attracts other kinds of community investments. A vibrant retail sector, including a full service grocery store, also promotes healthy behaviors and contributes to increased social capital.
Hazardous working conditions and low wage jobs, on the other hand, can threaten the health of community residents in many ways. Poverty is among the strongest determinants of poor health and is closely tied with low educational attainment and other threats to personal and community well-being. Concentrated poverty (geographical areas with high levels poverty) is associated with high levels of stress and risky coping behaviors, such as tobacco use and substance abuse. Communities without a strong economy and financial and job security are at risk of a host of poor health outcomes.
Hazardous working conditions and low wage jobs, on the other hand, can threaten the health of community residents in many ways. Poverty is among the strongest determinants of poor health and is closely tied with low educational attainment and other threats to personal and community well-being. Concentrated poverty (geographical areas with high levels poverty) is associated with high levels of stress and risky coping behaviors, such as tobacco use and substance abuse. Communities without a strong economy and financial and job security are at risk of a host of poor health outcomes.
Sample Strategy
A living wage is defined as the minimum income needed to meet basic needs. It is generally thought to be higher than the minimum wage set by the federal government, which since the 1970s has been considered inadequate for workers to live at a safe and sufficient standard of living. Living wage ordinances have emerged in response to the declining “real value” of the minimum wage. The basic philosophy behind the living wage movement is that someone working full-time should not be poor (PolicyLink, 2002).
The first living wage provision in the U.S. was passed in Baltimore, Maryland in 1994. By 2007, there were at least 140 living wage ordinances in U.S. cities and more than 100 living wage campaigns underway in other cities. Living wage policies typically require that local governments pay, and can only contract with companies that pay, a living wage. Therefore, living wage provisions apply to companies that provide municipal services and those receiving any government subsidies or financial assistance. There are several advantages to living wage provisions, including:
The first living wage provision in the U.S. was passed in Baltimore, Maryland in 1994. By 2007, there were at least 140 living wage ordinances in U.S. cities and more than 100 living wage campaigns underway in other cities. Living wage policies typically require that local governments pay, and can only contract with companies that pay, a living wage. Therefore, living wage provisions apply to companies that provide municipal services and those receiving any government subsidies or financial assistance. There are several advantages to living wage provisions, including:
- Improving living standards;
- Encouraging governments to employ local workers on public projects, instead of sub-contracting to the lowest bidder;
- Alleviating poverty;
- Reducing the strain on government welfare programs; and
- Stimulating the economy.
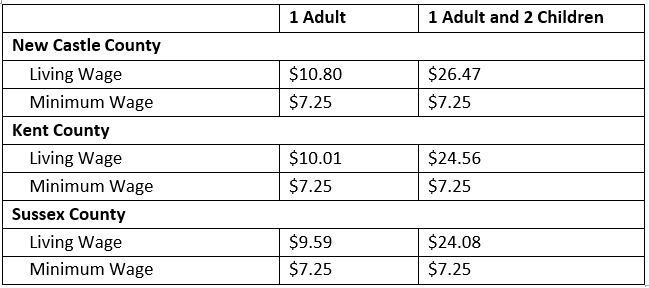
Table 3. Hourly Rate that an individual must earn to support their family, if they are the sole provider and are working full-time, in Delaware, in 2013
Source: Glasmeier, 2014
Unfortunately, in 2015, a living wage campaign is not high on Delaware’s legislative agenda. However, other efforts are underway to improve the economic environment, which may alleviate some of the disadvantages of living on minimum wage. For example, the Blueprint Communities Program is helping to build economically, physically, and socially vibrant neighborhoods in several communities by developing the capacity of community stakeholders to plan and implement comprehensive revitalization plans. Blueprint Communities throughout Delaware include: Edgemoor Gardens, Simonds Gardens, Historic Overlook Colony and Vicinity in New Castle County; Wilmington’s Browntown, Eastside, 2nd District, Westside/Little Italy and Riverside communities; Dover; and the Town of Georgetown.
“Blueprint Communities” is an initiative of the Federal Home Loan Bank (FHLB) of Pittsburgh, which selected the University of Delaware’s Center for Community Research and Service (CCRS) as its partner to develop and lead the comprehensive training, coaching, and capacity-building program in Delaware. CCRS provides training, technical assistance, and coaching to self-developed teams comprised of community leaders, bankers, public officials, developers, and health and social service providers. The training aims to help them learn how to develop community revitalization plans that include implementable projects. The CCRS trainings enable the teams to obtain new knowledge and skill sets while engaging them in leadership development. Teams produce well-developed written plans with feasible projects that will improve their communities economically, physically, and socially.
Launched in 2008, the Blueprint Communities Program realized many positive impacts within its first two years. That success includes the development of nine plans which triggered more than $27 million in community development programs; the construction or rehabilitation of 118 housing units; 10 infrastructure improvements; and the launch of six other community projects. As a result of these changes, the FHLB of Pittsburgh committed $250,000 toward the affordable housing initiatives and $215,000 in business loans. The Delaware Community Investment Corporation, the Delaware Community Foundation, several local banks, and the Jessie Ball du Pont Fund provided another $325,000 in grants (FHLB, 2011). An important focus of the Blueprint Community planning teams is to include employment opportunities for members of their various communities in the projects and programs designed in their revitalization plans. Since 2010, several full and part-time jobs, with salaries above minimum wage, were created and sustained through Blueprint Community project or program implementation. Additionally, in three of the Blueprint Communities, access to fresh, healthy produce is another strategic focus resulting in the establishment of community gardens and small businesses.
Ultimately, however, an increase in the minimum wage is necessary to improve the state’s economic conditions for Delawareans to thrive and achieve optimal health. This can be accomplished through living wage campaigns and ordinances. For examples of living wage efforts, as well as guidance for ways to develop a living wage campaign, click here.
“Blueprint Communities” is an initiative of the Federal Home Loan Bank (FHLB) of Pittsburgh, which selected the University of Delaware’s Center for Community Research and Service (CCRS) as its partner to develop and lead the comprehensive training, coaching, and capacity-building program in Delaware. CCRS provides training, technical assistance, and coaching to self-developed teams comprised of community leaders, bankers, public officials, developers, and health and social service providers. The training aims to help them learn how to develop community revitalization plans that include implementable projects. The CCRS trainings enable the teams to obtain new knowledge and skill sets while engaging them in leadership development. Teams produce well-developed written plans with feasible projects that will improve their communities economically, physically, and socially.
Launched in 2008, the Blueprint Communities Program realized many positive impacts within its first two years. That success includes the development of nine plans which triggered more than $27 million in community development programs; the construction or rehabilitation of 118 housing units; 10 infrastructure improvements; and the launch of six other community projects. As a result of these changes, the FHLB of Pittsburgh committed $250,000 toward the affordable housing initiatives and $215,000 in business loans. The Delaware Community Investment Corporation, the Delaware Community Foundation, several local banks, and the Jessie Ball du Pont Fund provided another $325,000 in grants (FHLB, 2011). An important focus of the Blueprint Community planning teams is to include employment opportunities for members of their various communities in the projects and programs designed in their revitalization plans. Since 2010, several full and part-time jobs, with salaries above minimum wage, were created and sustained through Blueprint Community project or program implementation. Additionally, in three of the Blueprint Communities, access to fresh, healthy produce is another strategic focus resulting in the establishment of community gardens and small businesses.
Ultimately, however, an increase in the minimum wage is necessary to improve the state’s economic conditions for Delawareans to thrive and achieve optimal health. This can be accomplished through living wage campaigns and ordinances. For examples of living wage efforts, as well as guidance for ways to develop a living wage campaign, click here.
Service Environment
It is not surprising that high quality, accessible, and affordable health care services contribute to the health of a community. However, other kinds of services such as high performing schools, strong public safety, efficient public transportation, good sanitation services, churches, clubs, and recreational services also contribute to a community’s health. For instance, after-school programs and recreation centers provide space for social interaction and positive youth development. Senior centers offer similar opportunities for older residents to interact socially and promote physical activity. Sanitation services affect health directly by reducing environmental hazards and indirectly by promoting a clean and more appealing place to live and work. Good schools contribute to good health in many ways, including short-term effects on literacy and long- term impacts on employment and wealth. Similarly, efficient and accessible public transportation services can reduce reliance on fossil fuels, ease traffic congestion, and reduce air pollution while lowering residents’ transportation costs, promoting physical activity, and improving access to jobs and other community services. Additionally, public transit can simultaneously improve the social environment by promoting social ties.
A lack of any of these services can put communities at higher risk for poor health and often discourages investment, which inhibits other services from existing locally. For example, lack of adequate public safety services and sanitation can be linked to higher crime rates. Inaccessible and/or poor quality health care, or care that is not culturally appropriate, can contribute to poor outcomes because residents are unable to get appropriate treatment when they are ill. Communities without recreational services or community centers may lack opportunities for social interaction. Finally, communities that lack dependable public transportation cannot link residents with jobs or other community services. Overall, deficiencies in the availability and quality of services prevent communities from attaining optimal health.
A lack of any of these services can put communities at higher risk for poor health and often discourages investment, which inhibits other services from existing locally. For example, lack of adequate public safety services and sanitation can be linked to higher crime rates. Inaccessible and/or poor quality health care, or care that is not culturally appropriate, can contribute to poor outcomes because residents are unable to get appropriate treatment when they are ill. Communities without recreational services or community centers may lack opportunities for social interaction. Finally, communities that lack dependable public transportation cannot link residents with jobs or other community services. Overall, deficiencies in the availability and quality of services prevent communities from attaining optimal health.
Sample Strategy
Transit-oriented development has been described as “a planning and design trend that seeks to create compact, mixed-use, pedestrian-oriented communities located around new or existing public transit stations” (Policylink, 2008). Transit-oriented development has grown tremendously over the past several years, and the approach is highly regarded because it contributes to healthy communities. However, transit-oriented development without adequate attention to equity can lead to gentrification and displacement of lower-income residents. Community engagement in the transit-oriented development planning process is critical. Many Community Development Corporations are now facilitating this approach and empowering communities to take the lead. For examples of community-led transit-oriented development that promote health equity, including strategies, challenges, and recommendations, click here
Delawareans have paid considerable attention to transit-oriented development in recent years, even including it in a broad effort to promote “Complete Communities.” Complete communities are livable, sustainable, and meet the needs of people of all ages, abilities, ethnicities, and income levels. According to Scott and colleagues (2010) from the University of Delaware’s Institute for Public Administration (IPA):
“A new vision for transportation policy and planning has emerged that includes a focus on community livability, transportation accessibility, and transportation equity. Livable communities integrate transportation and land-use planning to achieve more sustainable growth, development, and accessibility of residents. The new vision for transportation policy and planning also stresses the need to invest in transportation accessibility—or multi-modal transportation systems that serve people of all ages, abilities, ethnicities, and incomes. Transportation and land-use planning need to be assimilated to manage growth, focus on infill development, preserve community character, and provide equitable and accessible transportation options” (p. 1).
Such a comprehensive and integrated approach requires intersectoral collaboration and strong community engagement, similar to other health equity approaches described throughout this guide. In partnership with the Delaware Office of State Planning Coordination, the Delaware Department of Transportation, and the Delaware Association of Realtors, experts from IPA developed a “Complete Communities Planning Toolbox.” The Toolbox helps build local capacity to develop “complete communities” planning approaches, community design tools, and public engagement strategies. The Toolbox and related resources (including a review of best practices for complete communities) may be accessed here.
Delawareans have paid considerable attention to transit-oriented development in recent years, even including it in a broad effort to promote “Complete Communities.” Complete communities are livable, sustainable, and meet the needs of people of all ages, abilities, ethnicities, and income levels. According to Scott and colleagues (2010) from the University of Delaware’s Institute for Public Administration (IPA):
“A new vision for transportation policy and planning has emerged that includes a focus on community livability, transportation accessibility, and transportation equity. Livable communities integrate transportation and land-use planning to achieve more sustainable growth, development, and accessibility of residents. The new vision for transportation policy and planning also stresses the need to invest in transportation accessibility—or multi-modal transportation systems that serve people of all ages, abilities, ethnicities, and incomes. Transportation and land-use planning need to be assimilated to manage growth, focus on infill development, preserve community character, and provide equitable and accessible transportation options” (p. 1).
Such a comprehensive and integrated approach requires intersectoral collaboration and strong community engagement, similar to other health equity approaches described throughout this guide. In partnership with the Delaware Office of State Planning Coordination, the Delaware Department of Transportation, and the Delaware Association of Realtors, experts from IPA developed a “Complete Communities Planning Toolbox.” The Toolbox helps build local capacity to develop “complete communities” planning approaches, community design tools, and public engagement strategies. The Toolbox and related resources (including a review of best practices for complete communities) may be accessed here.
Please note that much of the content for the description of dimensions of PBIs comes from the publication Why Place Matters: Building a Movement for Healthy Communities, produced by PolicyLink in 2007.
3. Resources for Implementing Place Based Initiatives
Through its work as a designated World Health Organization (WHO) Collaborating Centre for Community Health and Development, the Kansas University Work Group for Community Health and Development created “The Community Tool Box” (CTB). This tool box is a comprehensive, online, and publicly available resource for people working collaboratively to build healthier communities.
Readers are highly encouraged to access the CTB and related materials. Each chapter has detailed sections describing key elements of the strategy along with related checklists, examples, and PowerPoint presentations. Associated toolkits include detailed instructions and examples. In addition to these resources, the CTB website includes a troubleshooting guide for identifying and addressing common problems in community health work as well as a database of best practices. There is an online course for community health promotion as well as an “Ask an Advisor” feature, which links users with community leaders and experts in the field. Furthermore, because health equity raises specific issues that warrant additional attention, some of the topics included in the CTB are discussed in greater detail in Section 6 (policy-oriented strategies) and Section 7 (data needs and evaluation approaches for health equity).
To ensure access to the necessary knowledge and skills needed to build healthy communities, the Kansas University Work Group for Community Health and Development made their community tool box widely available. The contents are exhaustive and include 46 chapters through which users can obtain practical, step-by-step guidance in community-building skills. The Table of Contents, including the major sections of the tool box, some sections are more relevant than others to specific communities and individual place-based efforts. However, it is valuable to see the extent of topics covered in the Community Tool Box, as this reflects the complexity of working with communities and the need for a different approach than what was traditionally used in health promotion and disease prevention.
Readers are highly encouraged to access the CTB and related materials. Each chapter has detailed sections describing key elements of the strategy along with related checklists, examples, and PowerPoint presentations. Associated toolkits include detailed instructions and examples. In addition to these resources, the CTB website includes a troubleshooting guide for identifying and addressing common problems in community health work as well as a database of best practices. There is an online course for community health promotion as well as an “Ask an Advisor” feature, which links users with community leaders and experts in the field. Furthermore, because health equity raises specific issues that warrant additional attention, some of the topics included in the CTB are discussed in greater detail in Section 6 (policy-oriented strategies) and Section 7 (data needs and evaluation approaches for health equity).
To ensure access to the necessary knowledge and skills needed to build healthy communities, the Kansas University Work Group for Community Health and Development made their community tool box widely available. The contents are exhaustive and include 46 chapters through which users can obtain practical, step-by-step guidance in community-building skills. The Table of Contents, including the major sections of the tool box, some sections are more relevant than others to specific communities and individual place-based efforts. However, it is valuable to see the extent of topics covered in the Community Tool Box, as this reflects the complexity of working with communities and the need for a different approach than what was traditionally used in health promotion and disease prevention.
Recommended strategies for implementing PBIs for health equity are consistent with evidence-based strategies for building healthy communities in general. An extensive body of literature is focused on the development of strategies for the implementation of PBIs. A comprehensive summary of resources is available and can be found here, as well as in section 4 of the guide.
"Building healthier cities and communities involves local people working together to transform the conditions and outcomes that matter to them. That civic work demands an array of core competencies, such as community assessment, planning, community mobilization, intervention, advocacy, evaluation, and marketing successful efforts. Supporting this local and global work requires widespread and easy access to these community-building skills. However, these skills are not always learned, nor are they commonly taught either in formal or informal education.” (Kansas University Work Group for Community Health and Development)
4. Recommendations and Lessons Learned
The Community Tool Box (CTB) developed by the Kansas University Work Group for Community Health and Development forms the basis of the recommendations presented in this section. We also include sample strategies because many of the “how to” strategies included in the CTB are not specific to health equity. Therefore, it is valuable to consider them within the context of recommendations and broad lessons learned from recent efforts to address health inequities for improving living conditions at the local level.
We have developed a list of recommendations and lessons learned, drawn from case study research conducted by PolicyLink (2007) and the Bay Area Regional Health Inequities Initiative (2013), as well as interviews with experts in the field (Knight, 2014). Some recommendations are reminders of important principles to keep in mind when promoting health at the community level using an equity lens. These recommendations build on the literature on health equities presented in the Background and Health Equity Lens sections. To access these recommendations, click on the button below .
We have developed a list of recommendations and lessons learned, drawn from case study research conducted by PolicyLink (2007) and the Bay Area Regional Health Inequities Initiative (2013), as well as interviews with experts in the field (Knight, 2014). Some recommendations are reminders of important principles to keep in mind when promoting health at the community level using an equity lens. These recommendations build on the literature on health equities presented in the Background and Health Equity Lens sections. To access these recommendations, click on the button below .
